
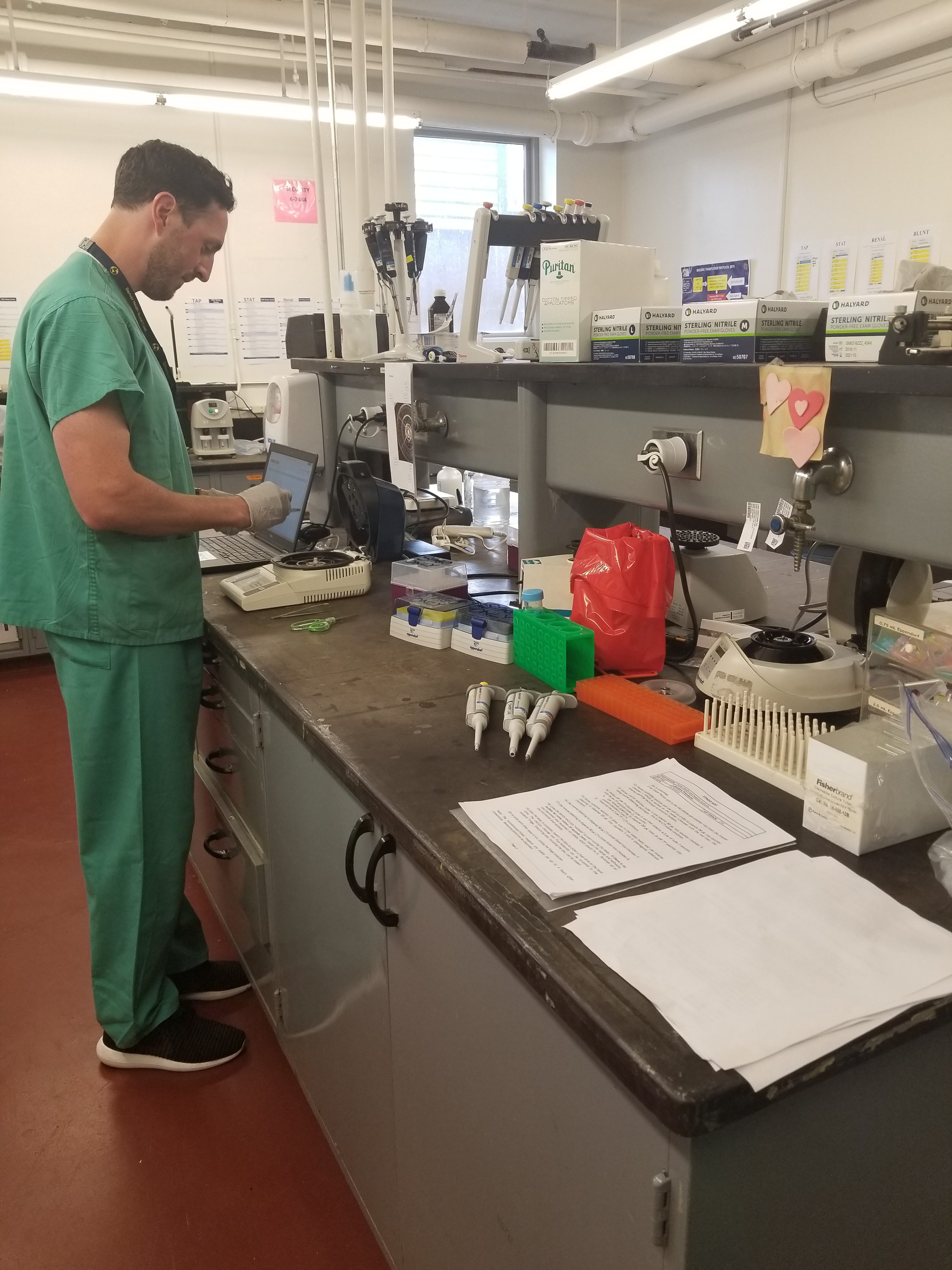
My first day was spent touring the hospital with Dr. Cohen and Alexis. We visited the trauma center, SICU (surgery intensive care unit), and surgery clinic. I spent the afternoon meeting with other members of the research team and talking to Alexis. Alexis took me to two labs, both testing blood, one of which belongs to Dr. Cohen.
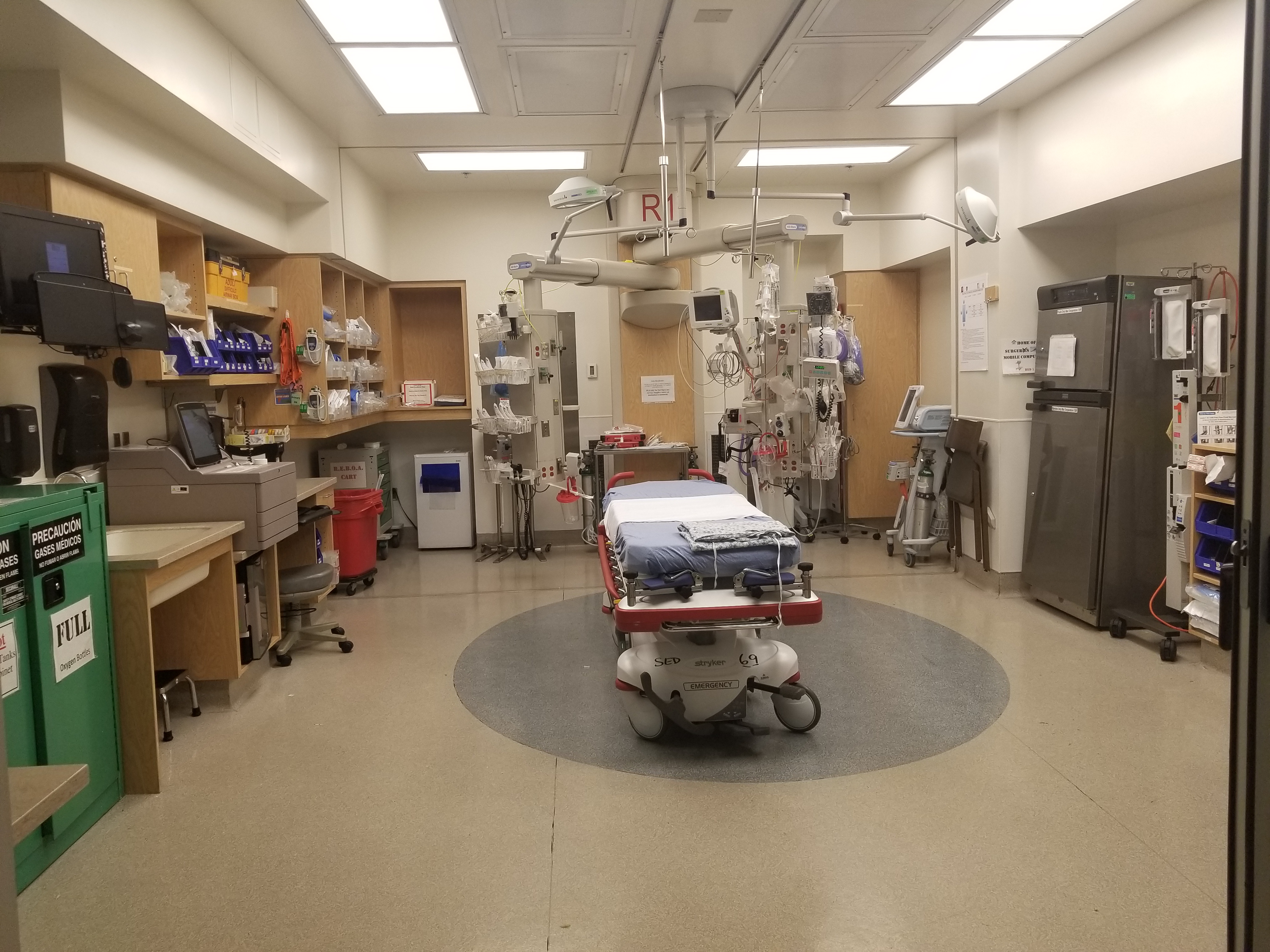
Second day, I was up early to “sign out,” or to meet with trauma surgeons and nurses to discuss patients from the previous night. They reviewed their diagnosis and plans for treatment, debated whether medications needed to be changed or the patient needed to be moved to the floor. I later spent an hour with neurosurgeons and nurses in the SICU, again reviewing current patients (called “Rounds”). Several patients suffered from brain hemorrhages, where a blood vessel rupture releasing blood in the brain. One patient had air in the front of his brain. Another suffered from a spinal fracture.
The rest of my morning consisted of two surgeries in the operating room. I shadowed Dr. Burlew, a scrub nurse, medical students, and a RN. The first surgery was a laparoscopic cholecystectomy converted to open. Dr. Cohen had me scrub in along with the other nurses and Dr. Burlew. The procedure began with slicing a small hole below the belly button, another on the right below his ribs, and on the left below his breast. Ports were placed in each hole. A camera went in the port below the belly button and on the left side. Dr. Burlew stepped in with her tools on the right side and they directed the camera to the gallbladder, which was swollen and oversized. Dr. Burlew couldn’t access the gallbladder, so they cut the hole on the right larger and disposed of the camera. They removed the gallbladder and proceeded to stitch the patient up. Once stitched and stapled, they woke the patient up and sent him back to his room to recover.
The next procedure lasted only thirty minutes. Once the patient was prepped and ready, the doctor and medical student began to cut a small incision on the patients left thigh. The doctor uses a scalpel to remove a portion of the patient’s muscle, transfers it to a wet cloth, seals it in a labeled tube, and then sends it to the lab to be tested. Again, thee, and then sends it to a lab to be tested. Again, the patient is stitched up and returned to his room to recover.
Later that day, I witnessed a younger patient enter the trauma center. She suffered from a fractured leg due to a motorcycle accident. The room was filled more than ten people, varying in occupation, rushing around taking notes, getting bandages, setting up her IV, getting x-rays, and informing her on the accident. She later got surgery on her fracture and will undergo physical therapy. Alexis and I didn’t stick around long as things dwindled down. We went with Conrad, who took samples of her blood, to the blood lab. We got several small vials of chemicals, and made four different test samples. Over the next two hours, we created four different tests. While the tests were processing, it was time for me to return back to my host home.
The next morning I spent time with Connor in the surgery clinic. We reviewed a patient’s documents, and then went to see him. This patient has a right inguinal hernia. He discussed the problem, listing symptoms of pain and pressure in the groin area, making daily tasks difficult. Connor then requested to see the hernia, pulling on gloves while the patient partially undressed. Connor slightly pressed on his hernia, pushing up and watching the bulge slowly disappear. Connor and I left the room to discuss treatments options with Dr. Cohen. Dr. Cohen went in, reviewing what Connor relayed. The patient repeated himself and Dr. Cohen took a look for himself. Dr. Cohen and Connor agreed that laparoscopic surgery in a few weeks is what would be best. They will take a piece of surgical mesh and stitch it to the weak spot of the scrotum. The flesh will scab over it, sealing the hole closed, preventing the intestines from protruding again. The second and third patients’ both have hernias, only the third’s was slightly different. He previously had a hernia about a year ago, with a large piece of mesh in the weak spot. He returned to the hospital, along with a new hernia. He was seeing whether it was a new one, or if the mesh came off. He refuses to get surgery, because that would be worse than dealing with the hernia, so the doctor told him to come back if his pain gets worse or he experiences vomiting or nausea.
My afternoon concluded with talking to Dr. Cohen and his colleague about a blood experiment. Dr. Cohen works in a blood lab outside of the hospital, running different tests and experiments. They reviewed the current experiment, tossing different ideas and changes to make next time and comparing graphs of each result. This experiment included one control and four variables, each variable with one of three different percentages: 10%, 15%, and 20% – resulting with twelve variables.
My last day at Denver Health started with a conference. CEO Robin Wittenstein gave a presentation about the hospital’s accomplishments and then focused on what Denver Health needs to focus on and work to achieve. She began with a brief intro, listing several subjects. She then proceeded to discuss each more specifically. Once her presentation was complete, people asked their questions.
Last hour of my internship was back at SICU. I spent time making rounds with the nurses and Dr. Campion. They took enough time to go over each patient’s medications, surgeries, symptoms, and overall wellness. They decided whether some things need changing, from changing meds to changing floors to sending them home.
During the second week for my internship, I learned more than I expected. Dr. Cohen and Alexis took their time to make sure I understood different diagnoses and complex procedures. My time spent at Denver Health increased my interest in the medical field and I look forward to learning more this year!



There are no comments published yet.